
From the 1Sunnaas Rehabilitation Hospital, University of Oslo, Faculty of Medicine, 2Department of Research, and 3Physical Medicine and Rehabilitation, Sunnaas Rehabilitation Hospital, Nesodden, Norway
Objective: To examine the effect of motion-controlled commercial video games compared with traditional occupational and physiotherapy methods for hand and arm function in persons of all ages with cerebral palsy.
Data sources: A systematic literature search was conducted in Medline, EMBASE, CINAHL, Cochrane Central Register of Controlled Trials, OTseeker and PEDro for randomized controlled trials involving persons with cerebral palsy using motion-controlled commercial video games as a training method for hand and arm function, compared with traditional therapy.
Study selection and data extraction: Screening, data-extraction, risk of bias and quality assessment was carried out independently by 2 of the authors. The risk of bias of each study was assessed using the Cochrane Collaborations Risk of Bias Tool. The quality of evidence was assessed using Grading of Recommendations Assessment, Development and Evaluation (GRADE).
Data synthesis: Eight randomized controlled trials, with a total of 262 participants, were included. A random effects meta-analysis showed a statistically significant difference compared to traditional therapy methods in favour of motion-controlled commercial video games. The quality of the evidence was, however, rated as very low.
Conclusion: Despite a significantly greater improvement in hand and arm function in favour of motion-controlled commercial video games, the results of this review should be interpreted with caution with regards to high risk of bias and the low strength of evidence. There is a need for high-powered studies on the effectiveness of training with motion-controlled commercial video games for persons with cerebral palsy, especially in adults.
Key words: cerebral palsy; video game; commercial video game; virtual reality; Nintendo; Xbox; PlayStation.
Accepted Nov 26, 2019; Epub ahead pf print De 3, 2019
J Rehabil Med 2020; 52: jrm00012
Correspondence address: Truls Johansen, Sunnaas Rehabilitation Hospital, University of Oslo, Faculty of Medicine, Nesodden, Norway. E-mail: uxjrul@sunnaas.no
The objective of this study was to examine the effect of motion-controlled commercial video games compared to traditional occupational- and physiotherapy methods on hand and arm function in persons with cerebral palsy. This review has investigated what the already existing Research have found on this subject and the results have been pooled to get a broader view of what effect this Method has for People living With cerebral palsy. The results of this study shows that motion-controlled commercial video games have a greater effect on hand and arm function compared to traditional therapy methods. Which means that motion-controlled commercial video games can be a good Method of training as an addition to traditional methods for therapists working with people with cerebral palsy.
Cerebral palsy (CP) refers to a category of multiple conditions of non-progressive neurological disorders, caused by damage to the brain in infancy or early childhood (1). In Norway, approximately 8,700 people are living with CP, and between 120 and 130 new cases of CP are registered each year (2). The prevalence of CP worldwide is estimated to be between 2 and 3 per 1,000 live births (1). CP can affect both cognitive and sensorimotor functions (3).
Approximately half of the persons diagnosed with CP have impaired upper extremity functioning, which includes grasping, reaching and manipulating objects (4). In addition, persons with CP mainly experience a more rapid physical decline compared with the non-affected population (5, 6). Due to these factors, persons with CP are in need of a lifelong exercise regime to maintain their physical functions. Because traditional physical exercise methods can become mundane and, in many cases, boring, it is crucial to find exercise activities that are motivating and fun to perform over time in order to maintain the desired levels of physical activity.
Motion-controlled commercial video games as a training method
In recent years, the rapid development of commercial gaming consoles, including motion-controlled video games (MCVG), has led to an increased use of such devices as physical training instruments. For persons with CP, MCVGs often offer an interesting and motivating training method supplementary to conventional training and physical therapy.
There are 2 types of video games available on the commercial market; games that utilize motion control (MCVG) and traditional video games that use hand controllers. Nintendo, Sony and Microsoft all produce their own motion-controlled consoles, with Sony PlayStation’s EyeToy being the first released in 2003. Nintendo’s Wii, introduced in 2006, was the first MCVG with motion detection in 3 dimensions.
A motion controller is a device that players can use to manipulate different objects on a screen by moving their bodies and thus control the game. MCVGs are suitable as physical training devices for persons with disabilities due to their ease of use. In the current meta-analysis, the focus will be on MCVGs. The use of MCVGs has increased proportionally with the technical evolution, including scientific studies that have shown MCVGs to improve motor functions as an alternative training method for persons of all ages with various neurological disorders, including CP (7). MCVGs are motivating because they are developed to be fun and employ gamification tactics, such as clearly stated goals, immediate feedback and rewards, which trick the user’s brain to want to play the game more (8, 9).
The different games in the selected studies challenge the player to use complex movements in their upper extremities in all 3 planes of movement. An example of such movement occurs when the player emulates a tennis swing, in which they use flexion in their elbow and shoulder, both internal and external rotation and abduction of the shoulder.
According to Lang and colleagues (10) a patient may achieve a rate of approximately 50 active movements per hour of traditional occupational therapy. On the other hand, some MCVGs have been shown to produce hourly rates of approximately 300 active movements (11). This may be attributed to MCVGs being designed to be fun and engaging, resulting in the player experiencing a state that resembles the flow of reality (12).
Multiple systematic reviews of the effectiveness of MCVGs among persons of all ages with CP have concluded that MCVGs may be as effective as traditional training methods on motor function, balance and strength (7, 13). The reviews contribute this effect to the motivational nature of the games used in the studies. A meta-analysis from 2018, which included 19 randomized controlled trials (RCTs) with a total of 504 participants with CP, found that virtual reality (VR) provided a strong effect (d = 0.861; 95% confidence interval (CI) = 0.51–1.22) on arm and hand function compared with other interventions. They also noted that engineer-built systems are more efficient than commercial consoles (14).
In addition to the results of studies of persons with CP, the rehabilitation potential of video games also has empirical support among other neurological conditions (15–18). This implies that MCVGs may be of benefit for the CP population.
Rationale for the present systematic review
As seen in the update of the Cochrane Review, from 2015 (19) to 2017 (16) the number of studies of stroke survivors more than doubled, which illustrates the need to also update the evidence on studies of CP in a field that is rapidly growing scientifically. A methodological concern with the available reviews and meta-analytical studies is the use of many different outcome measures and different devices that are not necessarily directly comparable. This systematic review is investigating a more homogeneous method of training, focusing only on MCVGs, namely Nintendo Wii (Nintendo, Kyoto, Japan), PlayStation Move (Sony Playstation™, Sony, Tokyo, Japan) and Xbox Kinect (Microsoft Xbox, Microsoft, Redmond, WA).
The aim of this systematic review is to synthesize the evidence for the effectiveness of MCVG training on hand and arm function in persons with CP, including children, adolescents and adults.
The specific research question is: What is the effectiveness of MCVGs as a method of training compared with traditional occupational and physiotherapy training methods for hand and arm function in persons with CP?
The Cochrane Collaboration’s method guidelines for systematic reviews were followed (20), and to ensure transparent and complete reporting of the review, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used to guide the process (21).
The protocol for this review was registered in PROSPERO (International prospective register of systematic reviews) on 29 May 2018 (identification number 98959).
Eligibility criteria
Eligibility was phrased using the PICOS approach (20):
Participants: Persons of all ages diagnosed with CP.
Intervention: Training with MCVGs, either Nintendo Wii or Wii U, PlayStation Move or EyeToy or Xbox Kinect.
Comparator: Traditional occupational and/or physiotherapy methods, such as neurodevelopmental training or task-oriented training or passive controls.
Outcome: Hand or arm function measured with an outcome measure that can be placed in the activity domain of the International Classification of Functioning, Disability and Health (ICF), such as the Quality of Upper Extremity Skills Test or the Jebsen–Taylor Hand Function Test.
Study design: Randomized controlled trials.
For inclusion in this study, the full-text articles had to be published in the Scandinavian languages or English. Exclusion criteria were: literature reviews and systematic reviews, studies with n < 5 subjects and studies performed before video games first started using motion controllers in 2003 (PlayStation EyeToy).
Systematic search of literature
One author (TJ) conducted the systematic search in January 2018; it was updated in May 2019 and one new study was identified. The electronic databases Medline, Embase, CINAHL, OTSeeker, PEDro and the Cochrane Central Register of Controlled Trials (Cochrane Library) were searched for both systematic searches.
The databases listed above were searched for eligible studies from the start of 2003 until May 2019. Specific search strategies were created in collaboration with a medical science librarian with expertise in systematic review searching and were peer reviewed by another independent medical science librarian according to the 2015 PRESS guideline statement (22) (Appendix SI1). Primary search terms used to define CP were: cerebral palsy, CP and cerebral palsies. Each of the primary terms was paired with secondary terms defining the intervention: video games, user-computer interface, exergame, game, gaming, Nintendo, PlayStation, Xbox, virtual reality, computer play, neurogame, Wii or Kinect. These terms were paired with a third set of terms related to measure outcome: upper extremity, upper limb, arm, hand, finger, wrist, forearm, shoulder or elbow. The search strategy was adapted to the syntax and subject headings of the different databases.The Medline search strategy is shown in Appendix SII1.
Study selection
After removal of duplicates, titles and abstracts were screened according to the eligibility criteria by 2 authors (TJ and JS) independently. The included references were retrieved in full-text, and reviewed again by the same authors; i.e. reviewed by one author (TJ) and double-checked by the second author (JS).
Data extraction and management
The extracted data were transferred to predefined summary tables by author TJ and verified by author POR. Extracted data included: type of video game device; specific games that were used; age, sex, and number of participants; GMFCS and MACS scores; duration of intervention; duration of intervention period; outcome measures; title, main author, publication year, journal name, country of origin, publication language; and setting. In cases where data needed in the meta-analysis were missing, the corresponding authors of the studies were contacted via email.
Risk of bias assessment
The risk of bias in the individual studies was assessed using the Cochrane Collaborations Risk of Bias Tool (20). To ascertain the validity of the included studies, 2 review authors (TJ and VS) independently assessed the risk of bias, judging the adequacy of randomization and concealment of allocation, the blinding of assessors and whether any suspicion of incomplete outcome data or selective reporting seemed likely. Any disagreement was resolved by a third author’s view of the assessment. Blinding of patients and healthcare providers was not possible due to the nature of the intervention. Risk of bias across studies was assessed using GRADEpro Guideline Development Tool.
Summary measures and synthesis of results
A random effects meta-analysis was conducted to synthesize the results. The choice of random effects was based on the heterogeneity of effect in our set of studies, the difference in the sample population considering that there was a range of participants from GMFCS I–V, and the use of multiple different outcome measures in the included studies.
Where the same outcome was measured using different, but comparable, tools on a continuous scale, the outcome measures were converted to a standard format by calculating the standardized mean difference (SMD) (Cohen’s d); i.e. the effect size (20). For reporting the results, the rule of thumb described by Cohen was used, which suggests that a SMD of 0.2 represents a small effect, 0.5 a medium effect, and 0.8 a large effect (23).
In studies that included multiple outcome measures for hand and arm function, a hierarchy system was established for the different outcome measures and data were added from the outcome measure highest on the hierarchy system. Two clinicians and researchers who were not involved in the study developed the system. Both have expertise in outcome measures regarding hand and arm function for people with CP. The system was designed to avoid risk of bias when pooling the results of 2 or multiple outcomes from a single study (24, 25).
In studies with missing data, the corresponding authors were contacted to request desired information; e.g. standard deviation (SD) for the difference in means. In cases where it was not possible to obtain this data, SD was imputed from p-values; a method recommended in the Cochrane Handbook for Systematic Reviews of Interventions (20).
In studies where p-values were not reported, correlation coefficients were calculated from other studies included in this review that utilized the same outcome measure, and these were used to calculate SDs from the reported difference in means, as recommended in the Cochrane Handbook (20).
Additional analyses
Two a priori subgroup analyses were performed. In order to investigate the effect of the duration of the intervention on the training effectiveness of MCVGs, a subgroup analysis was performed for 2 groups based on intervention length: studies with duration of interventions ≤ 6 weeks and studies with interventions > 6 weeks. To examine whether the type of console affects the results of the trials, a subgroup analysis was performed with 3 groups: studies utilizing Nintendo Wii, PlayStation 2, and Xbox 360, respectively. In addition, a post hoc subgroup analysis was performed to investigate whether the level of risk of bias influenced the results of the different trials. To do this, the studies were stratified into 3 groups: low, unclear and high risk of bias, as described in the Cochrane Handbook (20).
Study selection
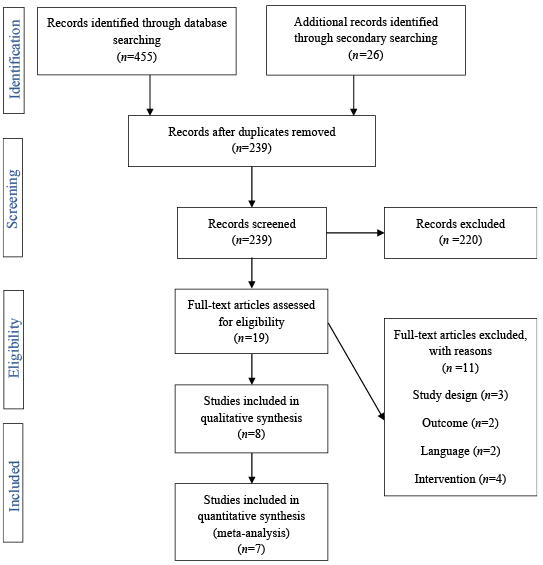
The primary search identified 455 references and the secondary search 26. After removal of duplicates, 239 references were screened. The full texts of 19 articles were read. A final total of 8 articles were included (Fig. 1). The characteristics of the excluded articles are shown in Table I. Reasons for exclusion were: the design was not a RCT (n = 3), the device used was not commercial (n = 4), the outcome could not be placed in the activity domain of the ICF (n = 2), or the study was not published in English (n = 2).
Fig. 1. Flow chart of identified, screened, excluded and included references.
Table I. Characteristics of excluded studies (n = 11)
Study characteristics
The study characteristics are summarized in Table II. All studies had a classic randomized controlled design, except for one, which had a randomized controlled crossover design (37). For the latter, the results after the first intervention period were used for the analysis. The included trials were published from 2008 through 2018. Of the 8 studies, 6 were conducted in a clinical setting (37–42) and 2 in a home setting (43, 44). The trials were performed in Egypt, India, Italy, the Netherlands, Saudi Arabia and Turkey.
Table II. Study characteristics. Intervention studies (n = 8)
Participants
The total number of participants was 262, with an age range of 5–20 years. All studies included both sexes. All but 2 studies (37, 40) included information about the participants’ gross motor functions and mobility through their Gross Motor Function Classification Scale (GMFCS) levels, which ranged from level 1 to level 5. Four articles (36, 39, 40, 42) included information about how the participants use their hands and how they manipulate objects, using the Manual Ability Classification Scale (MACS) level, also ranging from 1 to 5.
Intervention
The experimental interventions used in the trials were all commercial gaming consoles. Five trials used the Nintendo Wii (38, 40, 42–44), 2 used Xbox 360 (37, 39) and one used PlayStation 2 with EyeToy (41), all of which contain motion controllers or a camera that scans the user’s movements in order to play the games. Four trials used Wii Sport as the intervention (38, 40, 42, 44), one used Wii Fit (43), 2 used Kinect Sports and Kinect Adventures (37, 39) and one used EyeToy minigames (41).
One trial had an intervention period of 3 weeks (40), 3 trials had a period of 6 weeks (38, 41, 44), one had 8 weeks (37), 2 had 12 weeks (42, 43) and 1 had 16 weeks (39). Only one trial included a follow-up assessment, which was performed 12 weeks after after the end of the intervention period (44). Four of the studies had matched the dosage of intervention and swopped part of the usual therapy with MCVG training (37, 38, 40, 41), and 3 trials had MCVG training in addition to the usual therapy (39, 42, 44).
In 3 trials the participants performed the intervention twice a week (37, 38, 41), in 3 trials 3 times a week (39, 42, 44) and in 2 trials 7 times a week (40, 43). The duration of the intervention ranged from 15 to 45 min and the total amount of therapy provided varied from 6 to 108 h.
Comparison
One trial did not include a comparison intervention, but had a non-treatment group (43), and 2 trials used neurodevelopmental training (NDT) as the comparison (37, 38). NDT consists of guided or facilitated movements to ensure correlation of input from tactile, vestibular and somatosensory receptors within the body (45). The other trials reported that the control group received usual, regular or conventional therapy (CT). The CT included passive stretching, functional training, weight-bearing exercises, pegboard exercises and visual perceptual training.
Outcome
Each of the 8 trials used different outcome measures of arm and hand function that could be placed in the activity domain of ICF. Some of the studies had multiple outcome measures, therefore leading the meta-analysis to include 4 different outcome measures.
One study (43) was excluded from the meta-analysis due to lack of reporting of SD of the mean and p-values. After failing to establish contact with the corresponding author, no additional data could be extracted.
Risk of bias in individual studies
The assessment of risk of bias was performed at the study level and the studies were not blinded to the reviewers. The results are summarized in Figs 2 and 3.
Fig. 2. Risk of bias summary 1.
Fig. 3. Risk of bias summary 2.
Overall, there were many unclear and high risk of bias factors due to lack of reporting. Four of the 8 studies had adequate random sequence generation (39, 40, 42, 44), while 3 studies did not specify how the randomization was done (37, 41, 43). One study had a high risk of selection bias (38) due to a quasi-random design, in that the participants were divided into groups based on when they arrived at the clinic. Three studies specified how they concealed the allocation (39, 40, 42), while 4 studies did not explicitly report this (37, 38, 41, 43), 2 of which were judged to have a high risk of selection bias (38, 43). One study specified that the allocation had not been concealed and admitted that this could be a weakness in their study (44). Four studies did have a blinded outcome assessor (37, 40, 42, 44), while the other studies did not explicitly state whether they included blinded assessors. Two of this latter group (38, 41) were judged to have a high risk of detection bias when the outcome assessment was likely to have been influenced by the lack of blinding.
Five trials had complete outcome data (38, 40–42, 44), while 2 studies did not specify whether all the participants finished the trial (39, 43). One study had over 25% attrition and was judged to have a high risk of attrition bias (37). Four trials (37, 39, 42, 43) had a high risk of reporting bias due to reporting only subtests of different outcome measures and lacking SD on mean differences.
Blinding of participants and personnel was deemed impossible because of the nature of the intervention, and all studies but one (41) were therefore judged to have an outcome that was not likely to be influenced by lack of blinding.
Results of individual studies
Two studies (39, 42) reported statistically significant improvements in hand and arm function after the intervention period ended. Four studies (37, 38, 40, 41) favoured MCVGs compared with the control group, but did not report statistically significant improvements. One study (46) found no differences between the 2 groups.
Chiu and colleagues (44) had, in addition to the post-test at 6 weeks, a follow-up at 12 weeks. The participants had only their usual therapy in this period, but the content of the usual therapy was not specified. There was no difference between the 2 groups at follow-up.
None of the studies reported any adverse effects. El-Shamy and colleagues (42) reported that the compliance level in the experimental group was higher compared with the control group, which received the usual therapy, comprising passive stretching, weight-bearing exercises and task-oriented training.
Synthesis of results
A random effects meta-analysis was performed, which included 7 studies with a total of 222 participants. When comparing MCVGs with traditional training methods, a statistically significant difference was found between the 2 methods in favour of MCVGs, with an SMD of 0.89 (CI = 0.22–1.59), which indicates a large effect (Fig. 4).
Fig. 4. Forest plot of the effect of motion-controlled video games (MCVGs) vs traditional occupational and physiotherapy methods for hand and arm function in children with CP. 95% CI: 95% confidence interval, df: degrees of freedom; I²: measure of heterogeneity; Tau²: measure of variance; SD: standard deviation.
There was high heterogeneity among the studies, with an I² of 80%. The variance (Q = 30,72; p < 0.0001) indicates that the studies do not share a common effect. It was found that the heterogeneity was high because of 1 study (42), which showed a much greater improvement than the other studies. If this study was removed from the analysis, the heterogeneity decreased from high to low (I² = 8%), and the overall effect decreased from 0.89 to 0.47, which was still statistically significant (p = 0.003).
Subgroup analysis
The subgroup analysis of the type of MCVG resulted in 3 groups: studies that had used Nintendo Wii (38, 40, 42, 46), the one study that used the PlayStation 2 (41) and the ones that used the Xbox 360 (37, 39). No statistically significant differences between the 3 groups were observed (I² = 0%, p = 0.85). The greatest effect was, however, found for those utilizing the Xbox 360, with a moderate effect size of 0.70 (p = 0.007, 95% CI = 0.19–1.22) (Fig. 5).
Fig. 5. Forest plot of type of motion-controlled video game (MCVG). 95% CI: 95% confidence interval; df: degrees of freedom; I²: measure of heterogeneity; Tau²: measure of variance; SD: standard deviation.
The subgroup analysis of the duration of the intervention period revealed no statistically significant difference between the studies with an intervention period equal to or shorter than 6 weeks and those with longer than 6 weeks (I² = 47,2%, p = 0.17; Fig. 6). Studies with an intervention period longer than 6 weeks (37, 39, 42) had; however, a statistically significant total effect in favour of MCVGs (p = 0.05, CI = 0.02–2.77).
Analysis of the level of risk of bias resulted in 2 groups: high risk of bias and low risk of bias, as none of the studies were stratified in the unclear risk of bias group. The analysis showed no statistically significant difference between the 2 groups (p = 0.28; Fig. 7). The studies that were scored as having a low risk of bias (40, 42) had a high level of inconsistency (I2 = 92%, p = 0.0004), with a non-significant effect size of 1.77 (p = 0.13, CI = –0.52–4.06). The studies judged to have high risk of bias (37–39, 41, 46) only had a moderate degree of inconsistency (I2 = 25%, p = 0.26), with a significant effect size of 0.48 (p = 0.01, 95% CI = 0.10–0.86). The studies judged to have high risk of bias had higher homogeneity compared with the studies that had low risk of bias.
Fig. 6. Forest plot of duration of intervention period. 95% CI: 95% confidence interval; df: degrees of freedom; I²: measure of heterogeneity; Tau²: measure of variance; MCVG: motion-controlled video game; SD: standard deviation.
Fig. 7. Forest plot of duration of risk of bias. 95% CI: 95% confidence interval; df: degrees of freedom; I²: measure of heterogeneity; Tau²: measure of variance; MCVG: motion-controlled video game; SD: standard deviation.
Risk of bias across studies
The risk of bias across studies was assessed using the GRADE approach. The results of the assessment (Table III) show a very low quality of evidence, which indicates that any estimate of effect is highly uncertain. The downgrading was agreed upon by 2 of the authors (TJ and VS). The reasons for downgrading were the many unclear risks of bias, mainly in selection and attrition bias and high risk detected in selective reporting. Other reasons for downgrading were high heterogeneity explained by one outlier (42) and because the included studies had few participants.
Table III. GRADE evidence profile.
Question: Motion-controlled video games compared with traditional occupational or physiotherapy methods for hand and arm function in persons with cerebral palsy. Hand and arm function (follow up: range 3–16 weeks; assessed with: Quest; JTHFT; BBT; PDMS-2, MAUULF)
Our analysis, which included 7 RCTs and 222 participants, compared the use of MCVGs as a training method with that of traditional occupational and physiotherapy methods for hand and arm function in people with CP. The results show statistically significant improvements in favour of MCVGs.
These findings are similar to those of Ravi & Kumar and Chen et al. (13, 14), who reported that MCVGs may be as effective as traditional occupational and physiotherapy methods. One study (42) reported higher compliance in the MCVG group compared with the control group, suggesting that MCVGs are a motivating training method; a finding also reported in other studies (7). Chen and colleagues (14) found that engineer-built systems had a larger effect than MCVGs. However, such systems are not commercially available, are very large in size and are much more expensive than commercial MCVG, such as the Nintendo or Xbox platforms.
Even though we found a statistically significant effect in favour of MCVGs, the overall strength of the evidence is not sufficient to conclude with certainty the effectiveness of this training method. The results must be interpreted with caution due to several methodological concerns. The total number of included studies was small (n = 8), the studies included were relatively small, and the sample sizes varied, with only 1 of the studies (44) having more than 50 participants. Overestimation of treatment effect is more likely in smaller trials compared with trials with larger samples. Another factor was the different MCVG platforms, and specific differences regarding the devices applied. In Nintendo Wii, the user must hold a motion controller in their hand, while the Xbox 360 features hands-free play with Kinect, as the Kinect camera is able to detect motion without sensors. For people with CP with disabled hand and arm function, holding a controller may negatively improve the repetition rate. A higher number of repetitions has been reported to affect treatment outcome (47).
The studies varied when comparing the number of interventions per week, the duration of each intervention, and the intervention periods. This probably explains some of the variation in effect sizes between studies. The studies included a wide range of outcome measures, which were not always directly comparable. An interesting finding was that studies utilizing the Peabody Developmental Motor Scale – 2 (PDMS-2) as a measure of arm and hand function had a substantially higher effectiveness compared with studies with other outcome measures.
None of the trials elaborated on, or directly reported, whether the statistically significant improvement in the outcome measures actually improved activity and participation levels, including increased activities of daily living, functioning, and improved quality of life. None of the included studies discussed whether the mean difference of each outcome measure was a clinically relevant change, or how the result of the trials affected the participants’ everyday functioning.
Furthermore, only 8 studies were included in the current review, and only 7 could be included in the meta-analysis. These trials did not include enough patients to be able to draw firm conclusions about the effectiveness of MCVGs as a training method. All but one trial lacked follow-up testing to investigate the long-term effects of MCVGs, and this trial found no significant evidence of a long-term effect of MCVGs (44).
Limitations
This review has some limitations. The total number of studies included was small, the outcome measures varied across the studies and the participants had a wide range of functional capacities; all 5 levels of the GMFCS and MACS were included.
As regards the outcome measure, even though some studies utilized the same measure, others applied only parts of the test in their results, while other studies used the total scores. This may affect the validity of the measurements.
In addition, most of the studies had a small number of participants (n < 50), thus affecting the potential generalization of the results. Heterogeneity across the studies was high (I² = 80%), and it can be discussed whether it was appropriate to combine the results of the different studies or whether they are too dissimilar to compare. Because most of the heterogeneity was due to a single study (42), we considered it appropriate to combine the results of the different studies. There are many possible reasons why the participants in this single study improved more than those in other studies, but one reason may be that this study had the longest intervention period of all the included studies.
The risk of bias across the studies was high, with only one study having a low risk of bias on every domain scored. Compared with RCTs in other research fields (e.g. pharmacological studies), blinding the participants in studies of MCVGs and traditional training methods is deemed impossible.
Publication bias could account for some of the effect seen in this study, as we know that studies that show statistical significance towards the intervention investigated are more likely to be published than studies that show no effect (48).
In addition, this meta-analysis lacks studies of adults over the age of 20 years.
Conclusion
The results of this meta-analysis highlight the potentials of MCVGs as a supplementary method of training of arm and hand function for persons with CP. Even though a significantly greater improvement in hand and arm function in favour of MCVGs was found, the results should be interpreted with caution due to high risk of bias and the low strength of evidence. Despite these concerns MCVGs are a motivating, intensive and task-oriented training method that shows promising results.
Because persons with CP need lifelong exercise to maintain their motor functions, there is a need for high-powered studies with larger sample sizes and comparable outcome measures, on the effectiveness of training with MCVGs for persons with CP, especially in adults.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize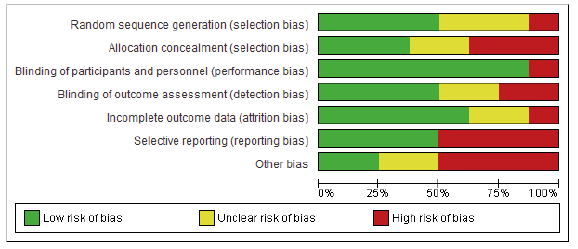 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize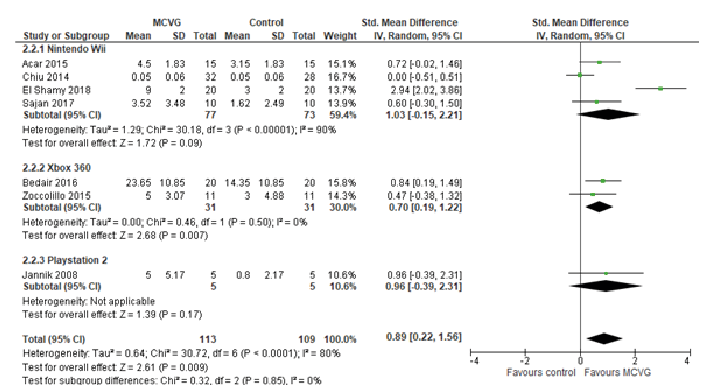 Click to show fullsize
Click to show fullsize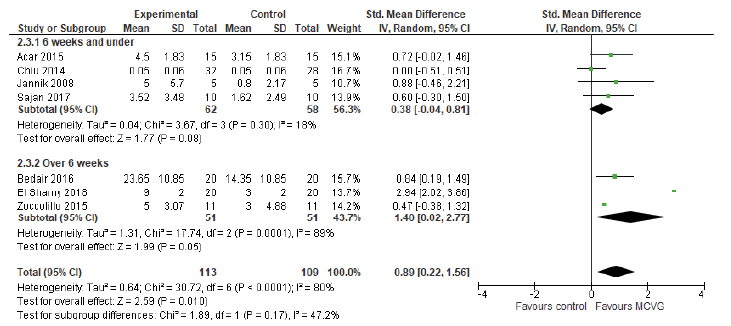 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize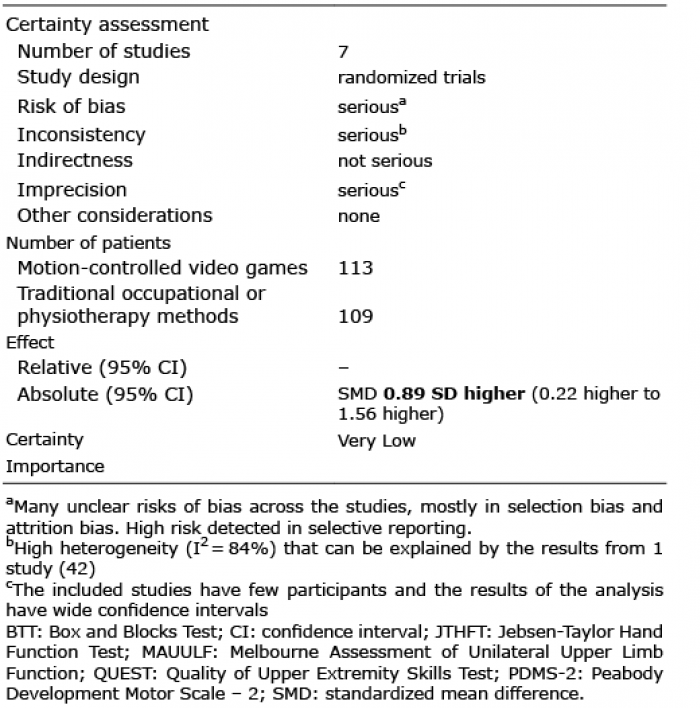 Click to show fullsize
Click to show fullsize